ConferenceSeries Ltd, USA extend a warm welcome to the distinguished Nobel laureates, speakers, delegates, palliative care specialists, health care community, palliative care physicians, geriatric physicians and Healthcare Industry leaders from around the world to Toronto, Canada, for attending Global Conference on Palliative Care during September 29-30, 2016 in Toronto, Canada.
We welcome and invite you to participate in our Premier event.
"Palliative Care 2016" aims to congregation participants from all Leading Universities, Clinical Research Institutions, Doctors, Nursing Professionals, Diagnostic Companies and Specialists in Health Care to share their experience and research aspects in the rapidly amplifying field and thereby, providing a showcase of the latest techniques in Emergency Medicine. We aim at understanding the intricacy faced by the relevant people of the industry and evolving towards a better charge in the field of Hospice and Palliative Care.
ConferenceSeries Ltd 1000+ Conferences Every Year across USA, Europe & Asia with support from 1000 more scientific societies and Publishes 700+ Open access journals which contains over 30000 eminent personalities, reputed scientists as editorial board members.
Track 01: Palliative Care and Hospice
Palliative care is an approach that boosts the quality of life of patients and their families facing the problem which correlates with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable estimation and treatment of pain and other problems, physical, psycho social and spiritual, whereas Hospice Care delineated to give supportive care to people in the final phase of a terminal illness and focus on comfort and quality of life, rather than cure. The objective is to enable patients to be comfortable and free of pain, so that they live each day as fully as possible.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences| Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care; Hospice and Palliative Care Association of New York State USA.
Track 02: Palliative Care and Symptom Management
Good administration of symptoms in the terminal phase is one of the main concerns of patients and their families. The physical amenity of dying patients requires thorough appraisal, excellent nursing care and careful prescribing. Some patients may experience unsuppressed and distressing symptoms at the end of life.
The palliative care accession to symptom management is based on thorough assessment of current symptoms, and planning ahead for common problems. There is adjuvant evidence from a systematic review which showed a small but consistent positive blow of palliative care services on symptoms, quality of life, and satisfaction at the end of life.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford USA; International Conference on Palliative Care.
Track 03: Palliative Care and Pain Management
Palliative care is a certain type of medical care that focuses on treatment of symptoms people may have when they are living with a chronic (longstanding) illness, such as cancer or heart failure. It is often compared to the hospice care that is extended to terminally ill people. In palliative care, the objective is to provide the best quality of life available even if someone is not terminally ill. Palliative care can be given when a person is assimilating treatment for a disease and when there is no useful treatment for the disease. However the majority of patients with cancer have pain, proper use of opioids and adjuvant drugs can provide adequate relief in most cases.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care.
Track 04: Palliative Care and Health Issues
Palliative care can address a broad range of issues, integrating an individual’s specific needs into care. The physical and emotional effects of cancer and its treatment may be very different from person to person. For example, differences in age, cultural background, or support systems may result in very different palliative care needs.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
International Aging summit August 08-09, 2016 Las Vegas, Nevada, USA;4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care; Hospice Program-Pennsylvania;.
Track 05: Palliative Care and Chronic Diseases
Chronic illnesses are marked by fluctuations and variations over time. Individuals with chronic illness experience pain and other symptoms that are not always adequately managed. Their caregivers often have to deal with enormous burden as the illness progresses. Palliative care can serve as an intervention to manage chronic illness, not just at the end of life but also in the early phases of illness.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care.
Track 06: Palliative Care and Non Malignant Diseases
Heart Disease identifies the need for patients with heart failure to have access to palliative care services for on-going support and advice; and for Renal Services goes further, listing as a quality requirement for patients near the end of life to have ‘a jointly agreed palliative care plan, built around their individual needs and preferences’. People with long-term neurological conditions, for example, should have access to a range of palliative care services when near the end of life.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
5th Geriatric Medicine Summit November 14-16, 2016 Atlanta, USA; 4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care.
Track 07: Palliative Care and Psychiatry
Palliative care psychiatry focuses on the emotional and social issues that arise in someone with an advanced illness, often in someone who is receiving hospice or palliative care (hospice being one end of the palliative care spectrum, which offers enhanced palliative care to patients with a short prognosis). Depression is highly prevalent in hospice and palliative care settings—especially among cancer patients, in whom the prevalence of depression may be 4 times that of the general population.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care; Hospice and Palliative Care Association of New York State USA.
Track 08: Palliative Care and Nutrition
Nutrition in palliative care and at the end of life should be one of the goals for improving quality of life. It is important to address issues of food and feeding at this time to assist in the management of troublesome symptoms as well as to enhance the remaining life. Cancer and its treatments exert a major impact upon physical and psychological reserves and at the end of life problems with appetite and the ability to eat and drink compound such impact. Identification of any nutritional problems can facilitate the employment of strategies which need to be discussed with the patient and their families and reviewed regularly as conditions change. Ethical questions will be raised concerning the provision of food and fluids to a person nearing the end of their life. Nurses need to acknowledge that food has greater significance than the provision of nutrients.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Congress on Geriatrics and Geriatric Oncology August 11-12 2016, UK; 4th International Geriatrics and Gerontology congress October 03-05 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care.
Track 09: Palliative Care and Paediatrics’
Paediatric palliative care is care designed to meet the unique and special needs of children living with life-threatening conditions such as cancer, muscular dystrophy, cystic fibrosis, severe brain problems, complications from prematurity and birth defects and rare disorders, among other conditions. It focuses on providing relief from the symptoms, pain, and stresses of a serious illness—whatever the diagnosis. The goal is to improve quality of life for both the child and the family.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Geriatrics and Gerontology Conference October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care.
Track 10: Palliative Care and Geriatrics
Geriatrics is a specialty that focuses on health care of elderly people. It aims to promote health by preventing and treating diseases and disabilities in older adults. There is no set age at which patients may be under the care of a geriatrician or geriatric physician, a physician who specializes in the care of elderly people. Rather, this decision is determined by the individual patient's needs, and the availability of a specialist. Geriatrics differs from standard adult medicine because it focuses on the unique needs of the elderly person. The aged body is different physiologically from the younger adult body, and during old age, the decline of various organ systems becomes manifest. Previous health issues and lifestyle choices produce a different constellation of diseases and symptoms in different people.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care; National Hospice and Palliative Care Organization Virginia USA;
Track 11: Palliative Care and Nursing
The goal of palliative care is to help them achieve the best possible quality of life through relief of suffering, control of symptoms, and restoration of functional capacity, while remaining sensitive to personal, cultural and religious values, believes and practices”. It is important that these nurses are trained in end of life treatment, psychological support, symptom management and enhancing the quality of life for their patients and the patient's families.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
3rd Geriatrics and Geriatric Oncology Summit August 11-12 2016, UK; 4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; Second International Aging and Disease Conference, October 01-02 2016, Stanford, USA; International Conference on Palliative Care; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA.
Track 12: Palliative Care and End of Life Care
Palliative care generally refers to patient and family-centred care that optimizes quality of life by anticipating, preventing, and alleviating suffering across the continuum of a patient’s illness. Historically, palliative care referred to treatment available to patients at home and enrolled in hospice. More recently, palliative care has become available to acutely ill patients and its meaning has evolved to encompass comprehensive care that may be provided along with disease-specific, life-prolonging treatment. End-of-life care refers to comprehensive care for a life-limiting illness that meets the patient’s medical, physical, psychological, spiritual and social needs. Hospice care is a service delivery system that emphasizes symptom management without life-prolonging treatment, and is intended to enhance the quality of life for both patients with a limited life expectancy and their families.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA; 4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA;
Track 13: Palliative Care and Terminal Care
Terminal care was defined as “the management of patients during the last few days or weeks or even months of life.” This vague definition makes visible the difficulties we have in estimating the duration of life for patients with end-of-life cancer. These difficulties can become an ethical dilemma when a physician, on referring a patient to a hospice programme, is obliged to predict accurately the patient’s prognosis.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; 21st International Conference on Palliative Care.
Track 14: Palliative Care and Emergency Medicine
Patients with serious or life-threatening illness are likely to find themselves in an emergency department at some point along their trajectory of illness, and they should expect to receive high-quality palliative care in that setting. In the last five years, emergency medicine has increasingly taken a central role in the early implementation of palliative care. Widespread integration of palliative care into the day-to-day practice of emergency medicine, however, is often jeopardized by the demands of many competing priorities.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Geriatrics and Gerontology Summit October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care.
Track 15: Palliative Care and Spiritual Care
Spirituality can be described as that which gives meaning to life. It refers to the universal human need for love, hope, relatedness, value, and dignity. Spirituality may or may not involve religious beliefs and practices. Learning that you or a loved one has a terminal illness presents many challenges. It can also present opportunities for life review, realized potential, celebration of accomplishments, connection with loved ones, and reconciliation. Hospice and Palliative Care are available to assist you with the challenges and opportunities that may arise. Palliative care is physical, emotional and spiritual care for a dying person when cure is not possible. It includes compassion and support for family and friends.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; International Conference on Palliative Care; International Aging and Disease Conference, October 01-02 2016, Stanford. USA.
Track 16: Palliative Care and Bioethics
Palliative care is a philosophy and a way of caring that aims to enhance the quality of life of patients and their families facing problems associated with life-threatening illnesses. The objective of palliative care is the prevention and relief of suffering by symptom control by integrating the Health Sciences with the Humanities.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA; 4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; 21st International Conference on Palliative Care.
Track 17: Palliative Care and Healthcare
Health care or healthcare is the maintenance or improvement of health via the diagnosis, treatment, and prevention of disease, illness, injury, and other physical and mental impairments in human beings. Health care is delivered by health professionals (providers or practitioners) in allied health professions, chiropractic, dentistry, midwifery, nursing, medicine, optometry, pharmacy, psychology, and other health professions. It includes the work done in providing primary care, secondary care, and tertiary care, as well as in public health.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
International Conference on Aging August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA; 4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; 21st International Conference on Palliative Care.
Track 18: Palliative Care and Alternative Healthcare
Complementary therapies are becoming increasingly used during the final stages of a condition, to enhance palliative or end-of-life care. These aim to help the patient cope with pain and the fear associated with the unknown, further decline, and death. These therapies include are designed to restore the body/mind balance and include things like aromatherapy, guided relaxation and imagery, music therapy, and therapeutic touch. They are thought to have a positive effect when it comes to helping the patient fall asleep, easing muscle tension, enhancing the effect of pain medication, enhancing rest, and relieving anxiety.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences| Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care.
Track 19: Palliative Care and Interventions
Palliative care at the end of life involves meeting the physical, psychological, social, and practical needs of patients and caregivers. It is not limited to the short period of time when the person is moribund. Good clinical care can prevent or alleviate suffering for many patients at the end of life by assessing symptoms and providing psychological and social support to the patients and their families.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Geriatrics and Gerontology Meeting October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; International Aging and Disease Conference, October 01-02 2016, Stanford. USA; 21st International Conference on Palliative Care. 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago;
Track 20: Palliative Care Management and Leadership
Research shows that palliative care and its many components are beneficial to patient and family health and well-being. A number of studies in recent years have shown that patients who have their symptoms controlled and are able to communicate their emotional needs have a better experience with their medical care. Their quality of life and physical symptoms improve.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care.
Track 21: Palliative Care and Oncology
Palliative care is any treatment that focuses on preventing and managing the symptoms of cancer and side effects of treatment. It also provides comprehensive support to people living with cancer and their families. Any person, regardless of age or type and stage of cancer, may receive palliative care.
Related Palliative care Conferences| Hospice Meetings| Geriatrics Conferences| Aging Conferences| Geriatric Medicine Conferences | Health care Meetings
4th International Conference on Geriatrics and Gerontology October 03-05 2016, UK; International Aging conference August 08-09, 2016 Las Vegas, Nevada, USA; 3rd Geriatrics and Geriatric Oncology Congress August 11-12 2016, UK; 5th Geriatric Medicine Conference November 14-16, 2016 Atlanta, USA, Hospice Program-Pennsylvania; National Hospice and Palliative Care Organization Virginia USA; 2016 AAHPM & HPNA Annual Assembly, March 9–12 Chicago; Hospice and Palliative Care Association of New York State USA ; American Geriatrics Society Annual Scientific Meeting, May 03-05 2016, Orlando, USA; Second International Aging and Disease Conference, October 01-02 2016, Stanford. USA; International Conference on Palliative Care.
Track 22: Entrepreneur Investment Meet
Palliative Care 2016 provides great avenues for Investors seeking for investment opportunities and expanding their business horizons. Our conference is attended by participants from more than 40 countries and attracts an interesting combination of academic researchers, practitioners and individuals who are engaged in various aspects of innovations in Palliative Care research thereby providing plenty of networking opportunities and newfound knowledge.
To explore more about business and investment opportunities write us at palliativecare@conferenceseries.com
Summary of Hospices and Palliative Care Conference (Overall Market of Hospices and Palliative Care with Statistics)
Hospices and Palliative Care Centers industry has evolved strongly over the past five years, while the outlook period through 2020 should be no different. Rising reimbursement from Medicare and Medicaid, coupled with an aging population, has propelled strong growth.
This multidisciplinary approach permits the palliative forethought group to address physical, passionate, otherworldly and social worries that emerge with progressed disease. Medications are said to have a palliative impact in the event that they diminish side effects without having a remedial impact on the underlying infection or cause. This can incorporate treating queasiness identified with chemotherapy or something as straightforward as morphine to treat the ache of broken leg or ibuprofen to treat yearning identified with a flu tainting. In spite of the fact that the notion of palliative forethought is not new, most medical practitioners have generally focused on attempting to cure patients.
Medicines for the easing of side effects were seen as risky and seen as welcoming fixation and other unwanted side effects. The focus on a patient's personal satisfaction has expanded significantly throughout the previous twenty years. In the United States today, 55% of clinics with more than 100 mattresses offer a palliative-mind program, and about one-fifth of group healing centers have palliative-mind programs. A generally later improvement is the palliative-mind group, a devoted social insurance group that is actually intended for palliative medication.
Scope and Importance of Palliative Care
Palliative Care is a zone of health care that keeps tabs on assuaging and anticipating the enduring of patients. Unlike hospice mind, palliative medication is suitable for patients in all sickness stages, incorporating those experiencing medicine for reparable ailments and those living with unending infections, and in addition patients who are nearing the close of life. Palliative prescription uses a multidisciplinary approach to patient forethought, depending on data from doctors, drug specialists, nurture, clerics, social laborers, analysts and other associated health experts in planning an arrangement of consideration to ease enduring in every aspect of a patient's existence.
Scope of Palliative care: A World Health Organization statement depicts palliative care thought as "a methodology that enhances the personal satisfaction of patients and their families confronting the issues connected with life-undermining disease, through the avoidance and help of enduring by method of unanticipated recognizable proof and faultless appraisal and medication of agony and different issues, physical, psychosocial and otherworldly." More by and large, in any case, the expression "palliative consideration" might allude to any forethought that mitigates indications, whether there is any expectation of a cure by different implies.Hence palliative medicines may be utilized to assuage the symptoms of therapeutic medications, for example mitigating the queasiness connected with chemotherapy. Provides help from ache, shortness of breath, sickness and other troubling indications. Palliative look after patients with any genuine disease and who have physical, mental, social, or otherworldly trouble as an aftereffect of the medicine they are looking for or receiving.
Palliative consideration expands solace by reducing agony, regulating manifestations, and decreasing stretch for the patient and family, and ought not be postponed when it is indicated. Palliative forethought is not saved for patients in close of-life consideration and can expand personal satisfaction and protract the patient's existence. In some cases, medical specialty professional organizations recommend that patients and physicians respond to an illness only with palliative care and not with a therapy directed at the disease. The following items are indications named by the American Society of Clinical Oncology as characteristics of a patient who should receive palliative care but not any cancer-directed therapy. Practice of Palliative care: -Evaluation of symptoms A method for the assessment of symptoms in patients admitted to palliative care is the Edmonton Symptoms Assessment Scale (ESAS), in which there are eight visual analog scales (VAS) of 0 to 10, indicating the levels of pain, activity, nausea, depression, anxiety, drowsiness, appetite and sensation of well-being, sometimes with the addition of shortness of breath. On the scales, 0 means that the symptom is absent and 10 that it is of worst possible severity. It is completed either by the patient alone, by the patient with nurse's assistance, or by the nurses or relatives.
WHEN TO CONSIDER PALLIATIVE CARE
-
Progressive declining health, despite treatment
-
Uncontrollable pain or symptoms
-
Shortness of Breath
-
Frequent hospitalizations
-
Repeat or multiple infections
-
Progressive weakness and fatigue
-
Decreased ability to perform personal (self) care
-
Change in mental status
-
Patient, family or caregiver’s stress
-
The desire of the patient and family to stop aggressive treatments
-
Difficulty with decisions about aggressive treatment
-
Uncertain goals of care
In the US palliative care services can be offered to any patient without restriction to disease or prognosis. Hospice care under the Medicare Hospice Benefit, however, requires that two physicians certify that a patient has less than six months to live if the disease follows its usual course. This does not mean, though, that if a patient is still living after six months in hospice he or she will be discharged from the service. Such restrictions do not exist in other countries such as the United Kingdom. Physicians practicing palliative care do not always receive support from patients, family members, healthcare professionals or their social peers for their work to reduce suffering and follow patients' wishes for end-of-life care.
Why it’s in Toronto, Canada
Toronto is the most populous city in Canada, the provincial capital of Ontario and the centre of the Greater Toronto Area, the most populous metropolitan area in Canada. In 2011, Toronto had a population of 2,615,060, making it the fourth most populous city in North America, after Mexico City, New York City, and Los Angeles. Classified as an alpha global city by the Globalization and World Cities Research Network, Toronto is a leading international centre of business, finance, arts, and culture, and is widely recognized as one of the most multicultural and cosmopolitan cities in the world.
The Toronto area has been inhabited for thousands of years by various Aboriginal peoples. The urban history of the city dates back to 1787, when British officials negotiated the Toronto Purchase with the Mississaugas of the New Credit. They established the Town of York, and later designated it as the capital of Upper Canada. During the War of 1812, York was ransacked and heavily damaged by U.S. troops in the Battle of York. The town was renamed and incorporated as the City of Toronto in 1834, and became the capital of the province of Ontario in 1867. Toronto occasionally expanded through amalgamation with surrounding municipalities throughout its history, the results of which can be seen in the 140 independently unique and clearly defined official neighbourhoods that make up the city.
Members Associated with Palliative Care
Some of the key players in this market segment are, the Jewish Family Service, the International Association of Geriatric Care, National Association of Professional Care Managers, and Senior Care Centers, the UF health, the World Health Organization and others. These players constantly participate in awareness programs, as well as mergers and acquisitions to serve the elderly society effectively.
Market Value on Palliative Care
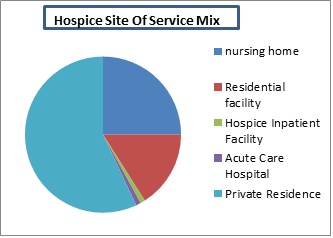
The overall shift towards treating patients outside of costly acute care settings benefits hospice utilization.98% of hospice patient care days are delivered in a non-acute setting.The percentage of elderly who died in acute care hospitals fell from 33% in 2000 to 25% in 2009.Patients and families continue to become more educated on the many benefits of hospice, driving utilization.
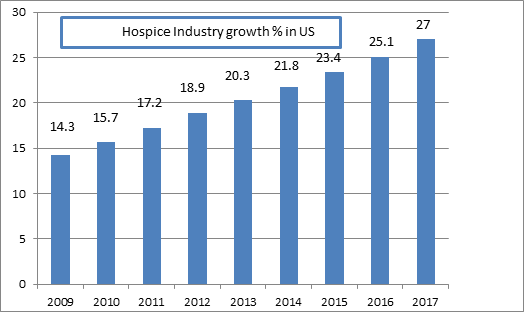
Market Growth of Palliative Care in the last and upcoming ten years
The $18.9 billion hospice industry is projected to grow 7.4% annually through 2017P.Hospice is the provision of holistic and individualized care to patients facing a life-limiting illness and their families. Congress created the Medicare hospice benefit in 1982.The goal of hospice is to maximize the quality of life and comfort, not to cure. Hospice is gaining wider acceptance as an alternative to curative care at the end of life. Approximately 44% of Medicare decedents in 2010 received hospice care compared to 23% in 2000.Growth in the hospice industry will be driven by shifts in patient preferences towards non-acute care, hospice’s cost saving value proposition, and the aging of the U.S. population.
Fund Allotment to Palliative Care
Hospice care, often covered by Medicare's hospice benefit, provides end-of-life care to a limited number of patients who are in their last six months of life. Most hospice care is provided on an outpatient basis, with routine home care the most common service10. The primary diagnosis of 63% of all hospice users includes, at least, one type of cancer, while the total number having some type of cancer is even greater 10, 45% of all cancer patients use hospice.
Hospice use is on the rise. From 1994 to 1998 hospice use by Medicare decedents increased from 11% to 19.3%. From 1998 to 1999, total hospice use increased almost 30% from 540 000 to 700 000 people11. The number of hospices has also increased, from about 1000 in 1991 to more than 2200 Medicare-certified hospices in 1998. The growth of hospice by Medicare decedents are increasing continuously year by year.
Statistics of Physicians, Researchers and Academicians working on Palliative Care Research
In total, 971 responses, including 293 from palliative care physicians, 112 from nurses, and 111 from chaplains, were received from 87 countries. Mean age was 48.5 years (standard deviation, 10.7), 64% were women, and 65% were Christian. Fifty-three percent reported their work as "mainly clinical," and less than 2.5% stated that no further research was needed. Integrating quantitative and qualitative data demonstrated three priority areas for research: Development and evaluation of conversation models and overcoming barriers to spiritual care in staff attitudes, Screening and assessment and Development and evaluation of spiritual care interventions and determining the effectiveness of spiritual care.


 Heidi Dowse
Heidi Dowse Ribereau Alexis
Ribereau Alexis Cordula
Cordula Amy Clements-Cortes
Amy Clements-Cortes Craig Omalley
Craig Omalley  Cordula
Cordula Amy Clements-Cortes
Amy Clements-Cortes Craig Omalley
Craig Omalley Kenichi Kume
Kenichi Kume Leyla Fallahi
Leyla Fallahi Akiko Nishikawa
Akiko Nishikawa Jaydeep
Jaydeep Michael Ian Rothenberg
Michael Ian Rothenberg Santhosh
Santhosh